
‘Choice’ has increasingly become a fundamental aspect of Western public health policy and practice since the late 20th century. For maternity care, it is a buzzword that has generated a growing body of research around how to best support decision-making and achieve informed choice among women. However, promoting more service user autonomy and care experiences that are aligned with personal values can lead to complex trade-offs, as choices are based on more sophisticated, expanding services with less reliance on a clinician’s intuitive judgment. While sometimes maternity care professionals believe they are offering choice, in reality, women still have a limited role in decision-making and do not feel their care is presented as a choice.
Is choice really so complex?
We often hear about the ‘burden’ of choice, and how difficult it can be to make one in complex situations or when there are many options before us. Long-standing understandings of decision-making and choice often assume that the decider uses a rational process to weigh up and decide between all available options. This idea of a ‘rational’ decision-making process is connected to classical decision theory, a concept developed during the 1950s. However, in reality, humans rarely make choices according to the standards of classical decision theory, even though the quality of their decision-making is judged based on the prescripts of this long-standing theory, despite its inadequacies.
Women’s decision-making and choice about pregnancy and birth care is a dynamic process.
‘Shared decision-making’ is a collaborative approach where clinicians support service users to reach a decision about their care. While shared-decision-making principles have been well-established, there are barriers to implementing them in practice.
Understanding decision-making and choice through research
Understanding decision-making and choice assumptions is important because there is growing evidence of the benefits of different options for maternity care in Western settings, as well as the notion of reproductive choice as a human right. As research studies increasingly collate evidence concerning the clinical outcomes of different care options, it should follow that we also bring together the findings about women’s experiences of choosing these options.
Reviewing a breadth of research all together can be helpful for elucidating complex phenomena, especially those that carry assumptions about what is optimal and what is not. Reviews also help researchers evaluate the quality of studies conducted on a specific area and determine whether there are any gaps in the literature. The aim of our review, published in BMC Pregnancy and Childbirth, was to describe and interpret qualitative research on women’s experiences of decision-making and choice about their pregnancy and birth care. Given the prominence of choice in health policy, we wanted to shed light on how this has been addressed in research to date and what the findings indicate.
Findings and conceptual model
We reviewed 37 original studies and conducted a meta-synthesis of these studies’ findings. A meta-synthesis involves bringing all of the qualitative data from a review together and re-analyzing it, in order to discover essential features across the body of literature. Because decision-making and choice are complex phenomena, we developed a conceptual model based on our analysis to bring all of these features together into one, presented in Figure 1:
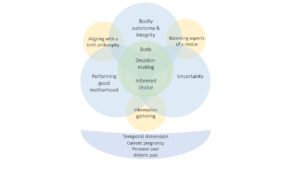
The model takes into account the three essential themes that emerged from the meta-synthesis:
- ‘Uncertainty’ encompasses several different experiences that are related to mothers’ concerns about the unknown and the course of pregnancy, childbirth and maternity care, all of which shape women’s decision-making and the options they ultimately pursue.
- Women frequently discuss their maternity experiences in terms of control, whether it be losing it, maintaining it or reclaiming it. We chose to shift the perspective to ‘Bodily autonomy and integrity’ because ‘control’ is not always explicitly stated by participants, and experiences often refer back to the body.
- ‘Performing good motherhood’ is related to responsibility and risk, which are often ascribed to mothers to manage, as well as the gendered cultural norm that ‘good’ motherhood and birth takes place in a hospital with a team of medical professionals.
The model also recognizes that decision-making is an active process, so these themes are connected through three inter-linking actions:
- ‘Information gathering’ illustrates the multiplicity of information-seeking and what women specifically gain from different sources.
- ‘Balancing aspects of a choice’ is concerned with looking at how women consider the different options available to them and, essentially, weigh the advantages and disadvantages of those they encounter.
- In terms of decision-making, an important part of the process is ‘Aligning with a birth philosophy’, or perspectives that inform the ways in which people understand the world and life in it, further shaping the information women access, the care opinions they ultimately choose and the ways they justify their choices.
An important finding from our review is that decision-making and choice are temporal, or related to time. For pregnancy and birth, they are made within a defined period, and often invoke both the past, whether this is personal, familial, social or historical, and the future. Finally, our discussion highlighted the importance of embodiment in maternal health experiences and how this is connected to experiences of decision-making and choice.
Conclusions and recommendations
Our findings indicate that women’s decision-making and choice about pregnancy and birth care is a dynamic process that is not always straightforward. This means that the use of prescriptive and rigid theoretical frameworks, like classical decision theory, for decision-making and choice need to be rethought. Policymakers and practitioners alike should examine critically current choice frameworks to ascertain whether they truly allow for flexibility in decision-making. Health systems should embrace more fluid, personalized models of care, such as midwife-led continuity models of care, to augment service users’ decision-making agency.

Comments