
Treating patients as individuals
There has recently been an enormous effort into developing a better prognostic classification for bowel cancer in order to enable us to better select patients for treatment. By classifying patients into smaller groups, we can select patients most likely to respond to a certain type of therapy resulting in an increase in response rates and minimizing unwanted toxicities. This is known as a precision medicine approach and in itself is not a new concept. In breast cancer, grouping patients by tumor characteristics to select the most appropriate treatment has been happening since the late 1980s, and in the early 2000s four breast cancer subtypes were defined which are still used in the clinic today.
Therefore, there remains a need to identify characteristics within both the tumor and surrounding cells which may not only guide prognosis, but also provide novel targets for adjuvant therapies. It is now recognized that from a genetic standpoint, as with many cancer types, CRC is not just one disease, but a heterogeneous group of cancers that arise within the same organ. Therefore, given their prognostic value, the ability to subtype patient tumors in the routine pathology setting would enable optimal treatment allocation.
Making it simpler
More recently this approach has been adopted by CRC scientists and in 2015 the leading experts in this field proposed four consensus subtypes for CRC. However, these four subtypes are dependent on specialized genomic testing, making them difficult and expensive for the clinical community to adopt. Therefore, we (Edwards research group, Wolfson Wohl Cancer Research Center, University of Glasgow) have performed a review of the literature (doi:10.1016/j.ctrv.2017.04.006) to identify features of the tumor that are easier to assess and devised a simpler method of subtyping CRC tumors that can easily be performed in routine diagnostic laboratory using existing techniques.
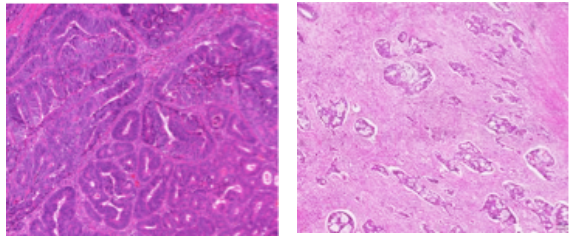
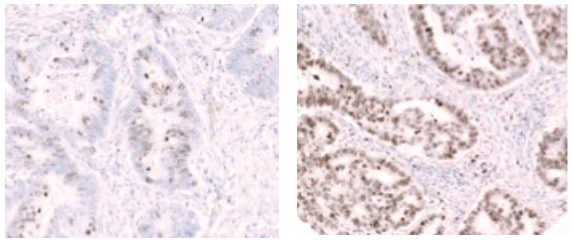
The subtyping method we propose is based on immune infiltrate, stromal invasion, and proliferation rate, all of which can be readily translated into routine pathology and is called phenotypic subtypes. Phenotypic subtypes classify patients into immune, stromal, canonical and latent subtypes.
The phenotypic subtyping method has been tested and validated in 3 retrospective different patient cohorts from across Europe (over 1000 patients) and a clinical trial cohort of almost 3000 patients. Excitingly not only can this subtyping method classify patients into different prognostic groups, but it is also associated with response to different chemotherapeutic regimens and therefore can be employed to identify which patient should receive which chemotherapy to maximize patient response and minimize patient’s toxicity. If this subtyping method can be incorporated into routine clinical practice it could revolutionize the treatment of patients, with different subtypes receiving different therapies. Currently we are working towards validating this within an international trial consortium (IDEA Trial) and if successful, we would then hope to test it in a prospective clinical trial.
Comments