
Consequences of community water fluoridation cessation
Community water fluoridation (CWF), the controlled addition of fluoride to a public water supply, has been described by the Centers for Disease and Control as one of the most positively impactful public health achievements of the modern day. CWF was first implemented in Grand Rapids, Michigan in 1945 and has since been employed across the United States and the wider world. CWF has been shown to significantly reduce childhood caries, the most common childhood disease.
This retrospective comparative analysis used dental claims records of 0-18 year old patients from Juneau (Alaksa) to explore the consequences of CWF cessation on dental health.
The effectiveness of CWF was confirmed by this investigation. The frequency of caries related procedures (particularly for 6-7 year olds) significantly increased during the fluoridation cessation period and there was an increase in the relative cost to treat the caries, suggesting an increase in caries severity.
CWF can be viewed as a kind of government investment which works towards protecting young people from childhood disease and school absences whilst simultaneously reducing government spending on healthcare claims.
Reporting of child maltreatment amongst public dental health personnel
According to the World Health Organisation, child maltreatment can come in the form of physical, sexual, psychological abuse, as well as generalized neglect. One quarter of adults worldwide were physically abused as children. Although abuse reporting continues to rise, an estimated third of victims of childhood sexual abuse cases go unreported. The importance of developing frameworks to detect potential hidden victims or at-risk children is immeasurable.
The repeated missing of dental appointments is considered to be an early indicator of struggling households and possible maltreatment.
In Norway, all children below the age of 19 are provided with free and regular dental treatments from the Public Dental Health Service (PDHS). The PDHS are required by law to report suspicion of child maltreatment to the Child Welfare Services (CWS). The CWS is required to respond to PDHS maltreatment concerns within 3 weeks, unless the concern is unsubstantiated. When PDHS concerns result in CWS investigation, the reporter is provided with outcome information.
1200 PDHS employees answered questionnaires regarding their reasons for sending a report to CWS and the responses the CWS gave. The most common reason for sending a report of concern was if a child did not attend a dental visit, and not direct suspicion of neglect or interaction with parents/guardians. The repeated missing of dental appointments is considered to be an early indicator of struggling households and possible maltreatment. Grave caries and a lack of hygiene came 2nd and 3rd on the list, respectively. 40% of PDHS reports of suspicion of psychological abuse and trauma resulted in CWS investigation and measures.
A quarter of reports resulted in measures, but the PDHS was not aware of the outcome of a third of submitted reports. Sexual abuse, grave caries and suspicion of neglect were the most strongly associated with CWS led outcomes. Although the PDHS were shown to be efficient reporters of potential maltreatment, the relatively low measures taken by the CWS, and even feedback to the PDHS , highlights a gap between the two organisations that requires some work to close.
Using machine learning to predict bad breath from the mouth microbiome
Oral malodour, otherwise known as halistosis, chronically affects around 50% of the developed world. It can lead sufferers to experience low self-esteem and bullying. The molecular culprits are volatile sulphuric and acidic compounds produced by periodontis-associated oral bacteria. Volatile sulphur compounds (VSCs) are produced by approximately 700 bacterial species residing in the human mouth. It is the concentration of the different compounds that each bacterial species produces, rather than presence of the species itself, which generates the resulting odour. For this reason it has been very difficult to establish a framework for predicting oral malodour.
To tackle this problem, the authors turned to Deep Learning, a machine learning process which is inspired by the communication patterns seen within the neurons of the human brain. Bacterial samples were taken from 90 patients, half with malodour and half without. Bacteria present in each sample were identified via 16s rRNA gene amplification and sequencing. This data, bacterial identity and the odour profile of individuals, was then sorted via deep learning.
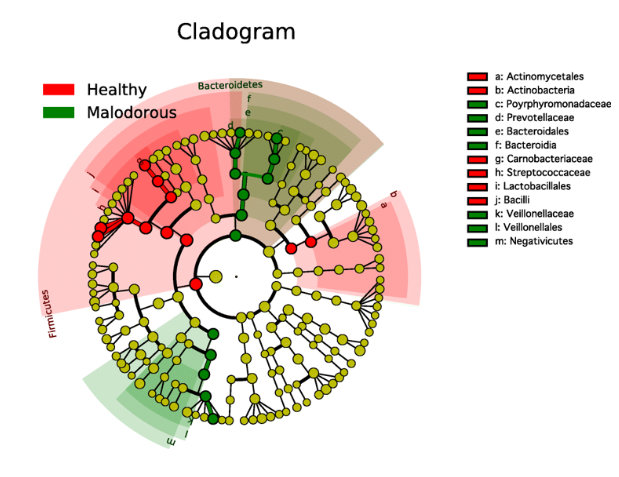
Healthy breath was associated with an abundance of Streptococcus, Granulicatella and Rothia, and malodour was associated with Veillonella, Peptostreptococcus, and Porphyromonas. The authors have provided evidence that saliva samples are a suitable substrate from which to assess oral malodour and have offered a potential deep learning based method in which the efficacy of malodour treatment can be measured.
The association between stress, saliva and dental caries
There has been much debate regarding the purported link between stress and the occurrence of dental caries. Stress can induce behavioural changes in people that can, in turn, be detrimental to oral health. A student’s tendency to increase sugar intake and neglect oral hygiene around exam time are examples of such behavioral changes. Stress can also induce flow rate changes in saliva. Behavioral and morphological changes collaborate to potentially increase the risk of dental caries amongst a stressed population.

In this scoping review, the authors performed a search in OVID, Embase, MEDLINE, PsycINFO, CINAHL, and WoS.
Six studies, which used cortisol as the biomarker of stress, were included in the review. 4 of these studies identified a link between salivary cortisol and caries, and the remaining 2 did not. The authors do not concede a causative link between cortisol and caries; however they instead identify cortisol and caries as an oral health research gap.
Regarding stress-induced salivary changes, the authors identify the limitation of the studies to have only measured acute stress responses instead of chronic stress exposure. The authors suggest the need for well designed, rigorous prospective cohort studies in which the extent that chronic stress (for example induced by low socio-economic status) effects caries is examined. The authors also suggest expanding cortisol-related measurements to more than just a single time-point (as seen in the examined studies) to better represent the complex factors contributing to human stress. The authors propose augmenting the measurement to also include:
1. The source of stress
2. The subject’s perception of stress
3. Physiological stress responses, for instance heart rate
The authors conclude that although evidence can be found to support links between stress and caries, the studies actually provide impetus for a pressing need for precise, detailed, methodologically sound studies.
Comparative effectiveness of school-based caries prevention
School-based caries prevention affords children greater access to dental care, and helps to homogenise the kind of care that children from different socio-economic backgrounds experience. School-based dental treatment involving the application of dental sealants is endorsed by The American Dental association. However, efficacy of such procedures has been identified as a knowledge gap and unexplored area of research by the Institute of Medicine (Washington, USA).
For this reason, the authors conducted a prospective observational study on 2 populations of children receiving school-based dental treatments. Both cohorts received glass ionomer sealants, but only one of the cohorts received a secondary intervention: interim therapeutic restorations placed on all asymptomatic teeth with carious lesions. Both interventions across both cohorts were performed every 6 months, and data was collected over the course of a decade.
Regarding teeth, examination of any decay, missing, filled, sound or pulpal abnormalities were noted. Variables such as pain, swelling, infection and abscess were also recorded. Data was collected by the dental hygienists and dentists performing these procedures in an e-Case Report Forms, which were electronically collated and analysed.
There was no statistically significant difference in the number of decayed or filled teeth across the cohorts. Interestingly however, there was a significant interaction between treatment and time, interpreted by the authors to mean that the incidence rate of decayed or filled teeth slowed over time for the children who received both primary and secondary interventions. This study offers important information to those involved in school-based optimal program design.
Comments